Dietary Fatty Acids: An Overview
Published on
This article was published in the November 2016 supplement edition of NHD magazine – I hope you enjoy reading about this much debated hot topic!
Fat is a macronutrient which our body needs in significant amounts to provide energy and also to aid the transport and absorption of fat-soluble vitamins (vitamin A, D, E and K)1. While some fats are essential to human health, others are associated with increasing the risk of chronic diseases such as heart disease when consumed in high amounts.
There is a lot of exciting research happening in relation to fats, which has simultaneously resulted in a lot of conflicting information surrounding this topic in the media. This article will aim to examine the current evidence base related to dietary fatty acids and summarise the main public health messages related to this.
A fat molecule is composed of a glycerol ‘backbone’ with fatty acids attached to this. Depending on the amount of hydrogen atoms present and the type of bonds present between molecules, these fatty acids are usually classified as: saturated, monounsaturated or polyunsaturated. Trans fatty acids occur when the carbon chains in polyunsaturated fats are arranged on opposite sides of a double bond rather than on the same side (which is known as a cis – arrangement and is found more commonly in nature than the trans-arrangement)2.

Picture source: British Nutrition Foundation “Fats”
Trans Fats
A high intake of trans fat is linked with a higher incidence of coronary heart disease due to raising LDL cholesterol and lowering HDL cholesterol3,4.
There are small amounts of naturally occurring trans fat found in some meat and dairy products such as: milk, cream, cheese, lamb, mutton and beef5. However the majority of trans fat is artificially produced when vegetable oils are hardened at an industrial level which turns them into a solid or semi-solid state (i.e. partially hydrogenated vegetable oil or fat) to use in processed foods for frying and baking or to improve the shelf life of the products such as: cakes, biscuits, pies, fried foods, margarine and takeaways2,5. There is currently insufficient evidence to differentiate between the health risks of naturally occurring trans fats and those which have been artificially produced6.
The best way to check if a product contains trans fat is to check the ingredients list for ‘partially hydrogenated fats or oils’; as fully hydrogenated fat does not contain trans fat. Many manufacturers have now altered their production methods in order to reduce the amount of trans fats in their products to very low levels5, and the most recent National Diet and Nutrition Survey (NDNS) found that average UK trans fats intakes where 0.5% of food energy, which is lower than previous years and remains below the recommended target of <2%7.
Saturated Fats
This type of fat is associated with raising LDL cholesterol levels and increasing our risk of heart disease1.
NICE report that a 50% reduction in saturated fat intake could potentially prevent 30,000 deaths from cardiovascular disease per year, and could also prevent a similar number of new cases from developing annually8.
Sources of saturated fat include: lard, butter, coconut oil, the visible fat on meat, full fat dairy, pies, pastries, cakes, biscuits, and takeaways1. It is recommended that saturated fatty acid intake should be <11% of total dietary energy; recent NDNS data shows that saturated fat intake for adults in the UK exceeds this at 12.7%7.
Saturated fat is currently a very hot topic and there are many contrasting opinions about how this nutrient effects our health; we will hopefully gain more clarity into this when the Scientific Advisory Committee on Nutrition (SACN) complete their review of the evidence related to saturated fat and health outcomes for the general population9.
A lot of the controversy arose with the release of a large meta-analysis by Chowdhury et al. (2014) which did not find a significant association between saturated fat intake and cardiovascular disease10.
Despite these findings and the numerous “Butter is Back” headlines, there have several criticisms of this study including: the omission of relevant studies in the meta-analysis, errors in the some of the data presented (with subsequent corrections by the author), a lack of consistency with the methodological approaches used in included trials (for example whether total fat or just saturated fat intake was reduced, and whether fat was substituted for refined carbohydrates), and it was highlighted that data representing monounsaturated fats was taken from meat and dairy rather than nuts, olive oil and plant sources11.
Other large scale meta-analysis’ which have accounted for some of these limitations found a reduced risk of cardiovascular disease as a result of lowering saturated fat intake, but not total fat intake, and replacing saturated fat with unsaturated versions or wholegrain carbohydrates, but not refined carbohydrates12-13. For example, a recent systematic review by Hooper et al. (2015)14 which included almost 60,000 subjects and trials which lasted at least 2 years, found that reducing saturated fat intake resulted in a 17% reduction in cardiovascular disease risk, and replacing saturated fat with polyunsaturated fat had a significant protective effect, whereas replacement with carbohydrate or protein was not found to be beneficial to health. They also found that reducing saturated fat intake was associated with improvements in weight and BMI.
Monounsaturated Fats
Monounsaturated fats are traditionally thought to be particularly beneficial for health via raising HDL cholesterol and lowering LDL cholesterol1,15; in line with this NICE recommends that those at risk of CVD should reduce their saturated fat intake and increase their intake of monounsaturated fats16.
Sources of monounsaturated fats include: olive oil, rapeseed oil, avocados, almonds, hazelnuts, peanuts1,17.
There has also been some emerging uncertainty related to the health benefits of monounsaturated fat as large scale data has reported that there is insufficient evidence to examine the effects of replacing saturated fats with monounsaturated fats14,18. Despite this uncertainty, there is an abundance of research to support the health benefits of wholefoods which are high in monounsaturated fats such as olive oil and nuts. For example, olive oil has an EFSA approved health claim that “consumption of olive oil polyphenols contributes to the protection of blood lipids from oxidative damage”19 and a meta-analysis by Schwingshackl & Hoffmann (2014)20 which included over 840,000 subjects found that a higher intakes of olive oil was associated with a reduced risk of all-cause mortality, cardiovascular events and stroke (by 11%, 12%, 9% and 17% respectively); but interestingly no significant association was found when monounsaturated fat was analysed in isolation. Similarly, a large meta-analysis by Psaltopoulou et al. (2011) found that the highest intakes of olive oil were significantly associated with a reduced risk of all types of cancer, and the authors conclude that it remains unclear whether this is related to olive oil’s monounsaturated fatty acid content or its polyphenol content21. In relation to nuts, randomised control trials have found that consuming a handful of nuts (roughly 40g) per day can reduce cholesterol levels by around 4%22-23.
It is interesting to note that the basis of the public health messages related to the benefits of monounsaturated fats is derived from studies such as the famous ‘Seven Countries Study’, the PREDIMED study and LYON heart study which found a reduced risk of the metabolic syndrome from following a Mediterranean diet, which included wholefoods which are high in monounsaturated fats, rather than from studying monounsaturated fat in isolation24-29.
Polyunsaturated Fats
Omega-3 (n-3) and omega-6 (n-6) are referred to as essential fatty acids as they cannot be synthesized in the body in sufficient amounts, therefore we must rely on dietary sources2.
There are 3 main dietary forms of omega 3: alpha linolenic acid (ALA), eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). ALA is a precursor to the active forms of omega 3 (EPA and DHA) which have important roles in building healthy cells, cellular signalling, reducing the risk of blood clots, helping to regulate heart rhythm, reducing inflammation, improving outcomes after a heart attack and may support good memory and help in the prevention and treatment of depression1,2,15,30. EPA and DHA can also be derived straight from dietary sources such as: pilchards, mackerel, herring, salmon, sardines and fresh tuna; whereas ALA is found in plant sources such as walnuts, rapeseed oil, flaxseeds, soya, dark green vegetables and wholegrain cereals (but ALA is thought to be poorly converted into EPA and DHA in humans)2,15.
For primary prevention of cardiovascular disease it is recommended to consume one portion (roughly 140g) of white fish per week and one portion of oily fish per week, and for secondary prevention it is recommended to consume two to four portions of oily fish per week (total 300g)15.
For those who are unable to tolerate oily fish, omega-3 fatty acid compounds or fish oil supplement are no longer recommended for primary or secondary prevention of cardiovascular disease due to a lack of supporting evidence31.
Linoleic acid is the main dietary form of omega 6 fatty acid, once consumed this is converted to the active form of omega 6 which is arachidonic acid (AA)32. The main sources of linoleic acid are vegetable oils such as: corn, safflower, sunflower and soya oils15,32, whereas preformed AA is found mainly in eggs, meat, and some kinds of fish31.
There is contention over the possible inflammatory effect of omega 6 in relation to coronary heart disease, as linoleic acid is used as a substrate for both pro-inflammatory and anti-inflammatory molecules. The American Heart Association (AHA) “supports an omega-6 PUFA intake of at least 5% to 10% of energy in the context of other AHA lifestyle and dietary recommendations [and] to reduce omega-6 PUFA intakes from their current levels would be more likely to increase than to decrease risk for coronary heart disease”32. However, a recent Cochrane review of randomised controlled trials reported that there is insufficient evidence to recommend altering omega 6 levels for cardiovascular disease prevention33.
Some research suggests that reducing the ratio of omega 6 to omega 3 in our diets could reduce the risk of cardiovascular disease; for example the western diet is thought to have a ratio of roughly 16:1 (omega 6:omega 3) whereas for secondary prevention of cardiovascular disease a ratio of 4:1 has been associated with a 70% decreased total mortality risk34, but more large scale data on this subject is needed. As discussed above there is also mounting evidence that replacing saturated fat with polyunsaturated fat reduces the risk of cardiovascular disease14.
Conclusion
Current evidence indicates that we should continue to limit our intake of trans fat and reduce our saturated fat intake (but not total fat intake), and replace this with unsaturated fat or wholegrain carbohydrates. There is a strong body of evidence to support the health benefits of the Mediterranean diet, including specific benefits of olive oil and nuts, but there is uncertainty around the direct effect of monounsaturated fat. Evidence to support the benefits of polyunsaturated fats is increasing, but more research is needed to explore the specific effects of omega 3 and omega 6 fatty acids.
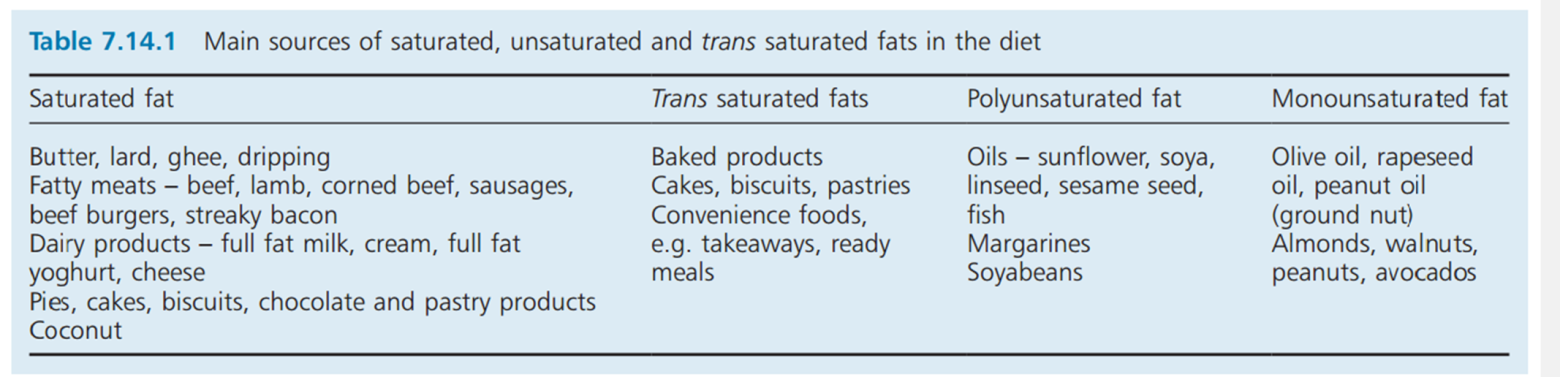
Table reference: Manual of Dietetic Practice (5th ed.)
References
- BDA (2014) Food Facts Sheet “Fats” https://www.bda.uk.com/foodfacts/FatFacts.pdf
- British Nutrition Foundation – Fats https://www.nutrition.org.uk/nutritionscience/nutrients-food-and-ingredients/fat.html
- Scientific Advisory Committee on Nutrition (2007) “Update on Trans Fatty Acids and Health”
- Department of Health (1994) “Nutritional aspects of cardiovascular disease”
- BDA (2014) Food Fact Sheet “Trans Fats” https://www.bda.uk.com/foodfacts/TransFats.pdf
- SACN (2007) “Update on Trans Fatty Acids and Health”
- Public Health England (2016) National Diet and Nutrition Survey Results from Years 5 and 6 (combined) of the Rolling Programme (2012/2013 – 2013/2014)
- NICE (2010) “Cardiovascular Disease Prevention”
- SACN (2016) Saturated Fats Working Group to Citations Received During the Call for Evidence
- Chowdhury et al (2014) “Association of Dietary, Circulating, and Supplement Fatty Acids With Coronary Risk: A Systematic Review and Meta-analysis”
- Annals of International Medicine (2014) http://wphna.org/wp-content/uploads/2014/08/2014-03_Annals_of_Int_Med_Chowdhury_et_al_Fat_and_CHD_+_responses.pdf
- Mensink et al (2003) “Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a meta-analysis of 60 controlled trials”
- Mozaffarian et al (2010) “Effects on coronary heart disease of increasing polyunsaturated fat in place of saturated fat: a systematic review and meta-analysis of randomized controlled trials”
- Hooper (2015) “Reduction in Saturated Fat Intake For Cardiovascular Disease”
- Manual of Dietetic Practice (5th ed.) “7.14 Cardiovascular Disease”
- NICE 2014 “Cardiovascular disease: risk assessment and reduction, including lipid modification”
- BDA (2014) Food Fact Sheets “Cholesterol” https://www.bda.uk.com/foodfacts/cholesterol.pdf
- Astrup et al (2011) “The role of reducing intakes of saturated fat in the prevention of cardiovascular disease: where does the evidence stand in 2010?”
- EFSA Journal 2011;9(4):2033 http://onlinelibrary.wiley.com/doi/10.2903/j.efsa.2011.2033/pdf
- Schwingshackl & Hoffmann (2014) “Monounsaturated fatty acids, olive oil and health status: a systematic review and meta-analysis of cohort studies”
- Psaltopoulou et al. (2011) “Olive oil intake is inversely related to cancer prevalence: a systematic review and a meta-analysis of 13800 patients and 23340 controls in 19 observational studies”
- Jenkins et al. (2002) “Dose response of almonds on coronary heart disease risk factors”
- Sabate et al. (2003) “Serum lipid response to the graduated enrichment of a Step I diet with almonds: a randomized feeding trial”
- Keys et al (1986) “The Diet and 15-Year Death Rate in The Seven Countries Study”
- De Lorgeril et al (1999) “Mediterranean Diet, Traditional Risk Factors, and the Rate of Cardiovascular Complications After Myocardial Infarction”
- Estruch et al (2013) “Primary Prevention of Cardiovascular Disease with a Mediterranean Diet”
- Salas-Salvado et al (2008) “Effect of a Mediterranean Diet Supplemented With Nuts on Metabolic Syndrome Status”
- Montserrat et al (2007) “Effect of a Traditional Mediterranean Diet on Lipoprotein Oxidation”
- Estruch et al. (2016) “Effect of a high-fat Mediterranean diet on bodyweight and waist circumference”
- BDA (2014) Food Facts “Omega 3” https://www.bda.uk.com/foodfacts/omega3.pdf
- NICE (2015) “Lipid-Modifying Drugs” https://www.nice.org.uk/advice/ktt3?unlid=7392292522016103135659
- Harris et al (2009) “Omega-6 Fatty Acids and Risk for Cardiovascular Disease”
- Al-Khudairy et al. (2015) “Omega 6 intake to prevent cardiovascular disease”
- Simopoulos et al. (2008) “The Importance of the Omega-6/Omega-3 Fatty Acid Ratio in Cardiovascular Disease and Other Chronic Diseases”











